A much-loved Labrador was referred to LPVS for investigation of a mass detected in her spleen by the primary care veterinary team, where she had presented for a loss of appetite and lethargy that was slowly getting worse over 3 weeks. During the clinical assessment at LPVS a new heart murmur was detected over the base of the heart, where the aorta and pulmonary arteries exit the heart. It was also noticed that 6 weeks previously she had brief episodes of lameness in different limbs. The lameness resolved but definitive causes had not been identified.
In order to assess the heart before further investigations were performed, and in order to make the general anaesthesia safer, the patients’ heart was examined by echocardiography, an ultrasound of the heart. From this we could see the leaflets of the aortic valve were extremely thickened, which resulted in the flow of blood out of the heart being restricted. The severity of the thickening of her aortic valve, along with changes in many of her blood tests, led to the diagnosis of Infective Endocarditis of the Aortic Valve. Unfortunately, her CT scan showed many blood clots around her body and an abscess in her spleen. Despite immediately starting on antibiotics, medication for her blood clots and pain relief, our lovely patient did not survive the night. She felt no pain, passing suddenly as she ate some ham with the nurses giving her lots of fuss and attention.
Infective Endocarditis, an infection on the valves of the heart, is an extremely rare condition in dogs, affecting <0.1% of dogs seen in referral hospitals. Currently the survival to 1 month has improved from 22% >20 years ago to 45%, as with most medicine early diagnosis and management is key.
Case details:
7-year-old FN Labrador presented to LPVS Surgical department for a possible splenectomy due to a 3cm mass on the tail of the spleen.
Over the previous six weeks there had been two episodes of lameness in different limbs that both resolved after a few days of NSAIDs and rest. In the previous 3 weeks she developed progressive hyporexia and lethargy.
On examination, a novel grade III/VI left base systolic and diastolic cardiac murmur was detected. Haematology demonstrated a moderate non-regenerative anaemia, mild neutrophilia with a left shift and moderate thrombocytopaenia. Biochemistry demonstrated mild hypoalbuminemia, moderate azotaemia, C-reactive protein >160 (0-10), Troponin I 28.9 ng/ml (0-0.2ng/ml) and NT-proBNP 4768 pmol/l (<900 pmol/l). Echocardiography demonstrated severe aortic valvular endocarditis with significant stenotic (average 68mmHg) and regurgitant flow. 4DX, Bartonella PCR and blood culture were all negative. Using the Modified Duke criteria, this patient had two major criteria; vegetative lesion and greater than trivial valvular insufficiency, and two minor criteria; new or worsening murmur and secondary disease, leading to the diagnosis of Infective Endocarditis (IE) of the Aortic Valve. CT demonstrated multiple thromboembolic lesions. The splenic mass appeared to be an abscess.
Treatment was started with broad spectrum antibiotics and clopidogrel. Unfortunately, this patient suffered a sudden cardiac death within a few hours of diagnosis.
Valvular endocarditis is a very rare condition in dogs, consisting of <0.1% of clinical cases within referral settings, and a high mortality rate of 55% within the first month following diagnosis, being reported despite medical management. Secondary disease such as neutrophilic polyarthritis, immune mediated haemolytic anaemia and thromboembolic disease is often associated with IE. Treatment involves broad-spectrum antimicrobials until blood culture results are available, antithrombotics due to the high risk of thromboembolic disease, and cardiac medications such as antiarrhythmics, diuretics or positive inotropes depending on the individual case. As with many conditions early diagnosis is key to improved outcomes.
If a patient has a novel cardiac murmur or a pre-existing valvular stenosis, alongside a wide range of other conditions; for example, shifting lameness, intermittent pyrexia, underlying neoplasia, surgical implants, immunosuppressive medication, chronic kidney disease or chronic waxing and waning symptoms, don’t forget to consider Infective Endocarditis in your list of differentials.
Quote/Clinician’s take-away or advice:
Kathryn Ling, RCVS AP in Veterinary Cardiology, asks one simple take away from this case, “Infective Endocarditis may be a rare condition but remember to auscultate all the heart valves in every physical examination and make a comment in your notes. The novel systolic and diastolic left cardiac base murmur was not detected prior to referral in this patient, as it was not audible of the left or right cardiac apex.”
Supporting Visuals:
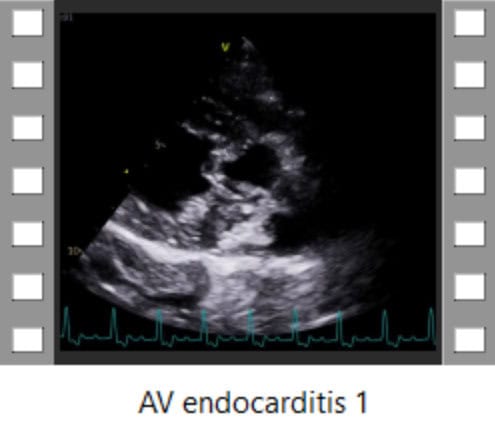
Right parasternal 5-chamber long-axis view demonstrating the significant vegetative lesions on the aortic valve leaflets.
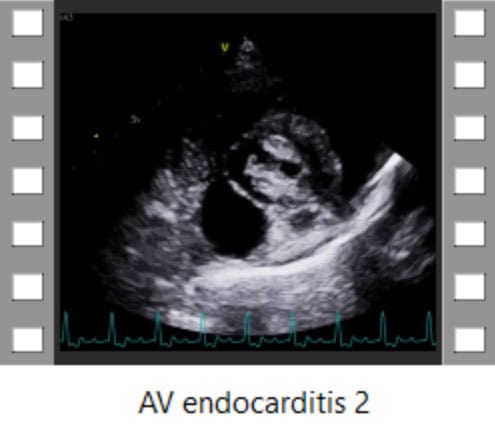
Right parasternal short axis view at the level of the aortic valve demonstrating the gross thickening of the aortic valve leaflets.
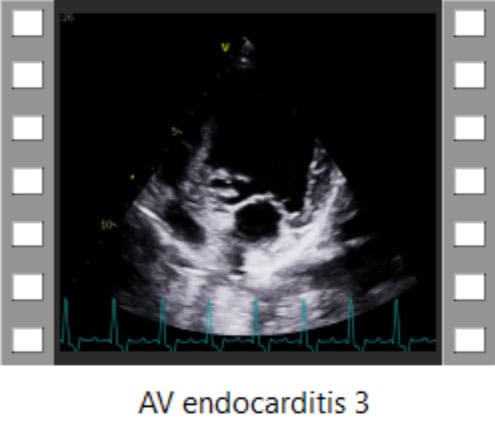
Left apical 5-chamber view of the left atrium, left ventricle, mitral valve and the significant aortic valve lesions, resulting in aortic stenosis and regurgitation.
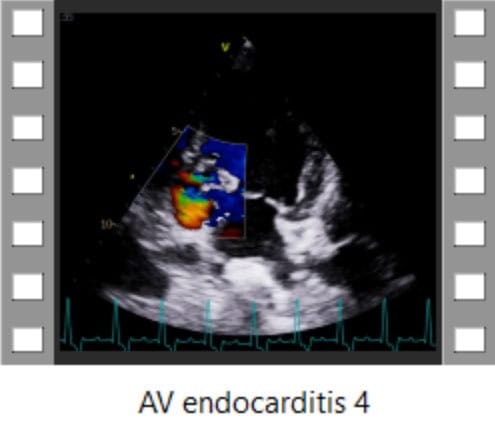
Colour-flow mapping Doppler demonstrating the aortic stenosis and regurgitation.