Summary:
Freyr presented to Lumbry Park in septic shock due to a perforated prostatic abscess.
This was a less common cause of septic peritonitis, which is typically due to gastrointestinal leakage secondary to a previous surgery. However, prostatic abscesses affect approximately 40% of male dogs with prostatic disease but they rarely rupture.
The outcome would almost certainly have been fatal if no treatment was given. The prognosis associated with this is generally quite guarded with a wide variation in reported survival rates, 50% on average.
Patient and issue summary
Freyr initially presented with an acute history of lethargy, vomiting, diarrhoea and bloody urine to his referring vets. He had a history of a chronic enteropathy. He deteriorated after initial medical treatment with intravenous fluid therapy, analgesia (paracetamol, methadone), antibiosis (potentiated amoxicillin) and anti-emesis (maropitant). By the time he arrived at Lumbry Park, he was collapsed in septic and hypovolaemic shock, which required stabilisation before he could be anaesthetised for diagnostic.
Examination and diagnosis
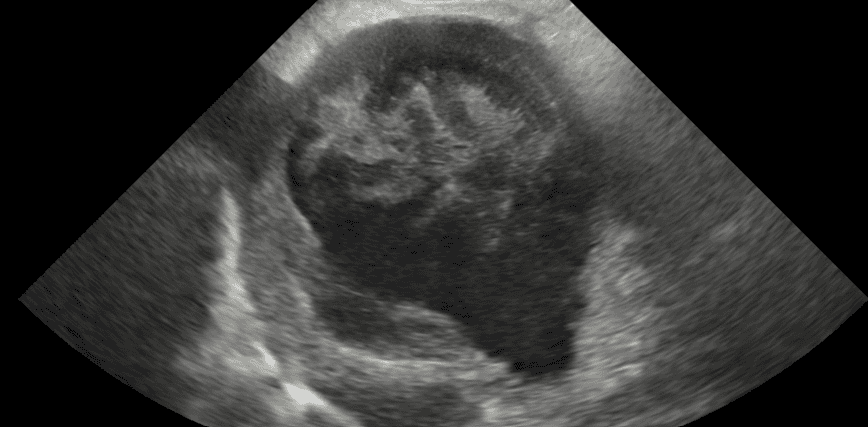
Ultrasonography was performed which was suspicious of prostatic abscessation and rupture with severe enteritis secondary to septic peritonitis.
Treatment
Freyr received intravenous fluid therapy boluses to improve his low blood pressure and stabilise him pre-anaesthesia. He required vasopressor medication almost from the outset of his general anaesthetic to support his blood pressure. He eventually became refractory to noradrenaline, dobutamine vasopressor therapy, and so was commenced on a hydrocortisone continuous rate infusion on suspicion of critical illness related corticosteroid insufficiency (CIRCI), which was successful. The surgery involved a midline laparotomy, prostatic debridement and omentalisation. Post-operatively, he was managed in intensive care, which included drainage of fluid from his abdominal drain and supportive feeding via an oesophagostomy tube. We also had the challenge of managing his marked postoperative ileus and regurgitation with a mixture of prokinetic and gastroprotectant medications.
Outcome and recovery
Freyr remained in intensive care for a few days before he could be discharged. He had developed acute kidney injury secondary to septic shock, which resolved with treatment. Freyr’s appetite improved so much after he had been sent home that he was eating too quickly and this was causing vomiting; this resolved with using a slow feeder.
“Freyr was such a lovely patient and it is so rewarding to see them do well when the prognosis can be so guarded. This is testament to the multi-discplinary approach we adopted to Freyr’s care; in particular, commencement of the hydrocortisone CRI appeared to be a turning point in managing Freyr’s blood pressure but there were lots of hurdles overcome along the way!” says Tom Hordle, Anaesthesia Resident at Lumbry Park Veterinary Specialists.
“Freyr is doing well and has matured since you saw him at Lumbry Park. He is a lovely family pet who enjoys playing with our grandchildren and running on Windmill Hill.”